Introduction
Distance education (DE) has become a popular option for expanding education and optimizing expenses but continues to be controversial. Evidence shows both positive and negative outcomes across educational fields, but the effect of DE in place of classroom instruction (CI) is equivocal (1, 2). Published literature on the subject frequently does not account for multiple experimental factors, such as the type of outcome measured, learner demographics, biased sampling, failure to put in place proper experimental controls, and confounding instructional methods that might affect outcomes, leading to potentially conflicting interpretations [1, 3, 4].
At the outset of this project, the U.S. Bureau of Labor Statistics occupational projections data suggested that employment of medical laboratory professionals was expected to grow by 14 percent between 2008 and 2018, faster than the average for all occupations. It projected that by 2018, the U.S. would need another 70,600 medical laboratory workers, with 20,500 at the baccalaureate level, to fill newly created positions, and 107,000 workers, 53,000 at the baccalaureate level, when considering replacement of retiring staff [5]. Each year, accredited programs graduated fewer than 4,700 laboratory workers, so to meet the workforce needs of the country, the number of graduates needed to increase more than twofold.
Of the more than 1,000 tests performed in the clinical laboratory, about 500 are used daily to help health care practitioners make decisions about disease prevention, assessment, diagnosis, treatment, and management, and provide 70-80% of the data used in clinical decision-making [6]. Clinical hematology is one medical laboratory field where identification of disease states by looking at patient samples under a microscope is critical. The ability to teach this skill has been dependent upon a student having access to both a physical specimen and a microscope with which to view it, each of which represent significant investment in effort and capital. These costs can be prohibitive when considering development or expansion of laboratory scientist education programs because the direct relationship between the number of students, microscopes and specimens is not amenable to new methods of teaching. With the advent of virtual microscopy, this relationship can be changed. However, the efficacy of teaching microscopy in a digital format has not been firmly established in undergraduate education, thus hindering development or expansion of laboratory science instruction that adopts virtual microscopy; ultimately restricting training to traditionally served demographic populations.
Changing Course Delivery
To address workforce shortage needs, our clinical laboratory sciences (CLS) program has begun to expand its program to one of its coordinate campuses 90 miles away. The expansion of our curriculum to this site created several challenges regarding the educational assets used to deliver the program. The capacity to teach medical laboratory scientists the skill of identifying disease states microscopically is limited by both the availability of physical samples relevant to laboratory science and by the lack of an environment in which alternative instructional methods can be objectively evaluated. Traditionally, undergraduate hematology morphology was taught using microscope slides where each student or a very small group of students had an instructional slide set. With our position in an academic health center, our instructional slide sets contain some of the rarest and most unique hematopathologies. However, glass slides can be damaged or broken and stains fade over time resulting in the loss of these precious resources that cannot be replaced. The challenge of delivering an equitable curriculum to distant locations along with the need to preserve our slide collection directed our effort to digitize the slide sets used in our teaching laboratories. We anticipate that this approach will play a central role in the distributed delivery of hematology through DE as new programs are initiated to address workforce shortage needs and expand undergraduate educational opportunities in laboratory science; ultimately increasing capacity to train much needed laboratory professionals and ensure continued quality of healthcare as demand increases with the aging population.
Despite the needs of our program, we were unsure whether digital microscopy would provide equivalent instruction compared to traditional face-to-face (F2F) delivery. The level of personal interaction and guidance provided during regular laboratory sessions seemed essential in developing the ability of students to distinguish subtle morphologic characteristics represented in varying disease states. Nevertheless, we recognized that delivery to alternate performance sites was not sustainable utilizing our limited number of teaching slide sets.
The digital slide library mimics the use of a real microscope and slide set where students can choose a disease entity or case and can view the associated slides at any magnification from 4X to 830X. These are not still pictures that students view to memorize specific cellular characteristics. Students can zoom in and out and move around, exploring the slides in a manner that assists their learning. Students encounter cells as they scan the slides and have to learn to recognize cells within the context of that particular pathology. Our students enjoyed the flexibility and access to the database that comes with DE and one student comment was that the course design surrounding the digital slide library enhanced their independent learning process. We evaluated the efficacy of virtual microscopy as the primary mode of laboratory instruction in undergraduate level clinical hematology teaching and found that students utilizing the digital slide database performed statistically better than those experiencing traditional face to face instruction [7].
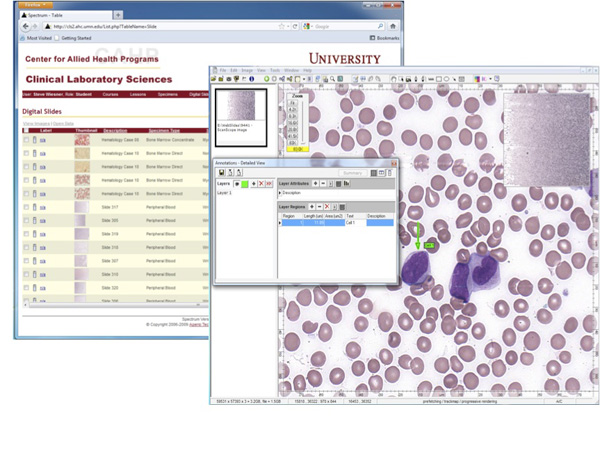
Figure 1. Screen shots of the image database and slide viewing software
Lessons from our experience
At the outset of this project, our program was grappling with the expansion of our curriculum to alternate performance sites without the necessary physical assets required for instruction. While we had done some preliminary investigation into the possibility of digitizing our microscope slide set, we did not have the resources necessary for completion of that task. We were fortunate that the opportunity for funding from the Learning Innovations Council at the University of Minnesota arose shortly after we had begun to consider this endeavor.
Having limited experience in development of digital educational resources, we grossly underestimated the amount of time that would be required to complete the project. This was mostly due to the age of our slide sets and the need to identify the best examples possible from our collection. Slides had to be individually marked to identify the area of the slide that displayed the relevant morphological characteristics. The slides were sent to our vendor for scanning, the files returned to us with the slides, images uploaded to the server and then converted to a format usable by software installed locally on the students’ computers. Once uploaded and converted, slides had to be properly identified, organized and annotated for student use.
In retrospect, this project was as much a coincidental confluence of resources as it was a planned effort. The technology was available commercially to enable digital delivery. The funding was available at the time of need. We had the need and desire to complete the project. That said, the single most important factor in the success of this project was the fact that we had identified the content to be delivered digitally before the other factors came into play. The first lesson learned in completing this project is that we must view our entire curriculum through the lens of digital delivery and identify the content that can be effectively conveyed to the students in a digital environment. The second lesson is that the digital environment used to deliver material must be tailored to the content. Content cannot be tailored to the environment. While tailoring content may be possible, ultimately the mismatch will result in less effective instruction for the student. Inevitably, the accommodations made to enable the content to be delivered in an inappropriate context will cause cumbersome changes that affect student learning. We were fortunate that we were able to take advantage of technology that had been commercially developed for digital microscopy and implement it in education. In spite of that fact, we continue to struggle utilizing digital microscopy software developed for clinical pathology as an educational tool. Limitations of the commercial software have forced us to find ways to work around features that are entirely justified in clinical practice but result in extra effort and wasted time in an academic teaching environment. As a result, some students have expressed frustration with these cumbersome procedures and it has dampened their enthusiasm for distance education. This should be a consideration when undertaking any transition to digitization and best efforts must be made to ensure that technology is not an impediment to learning, but an enhancement.
Impact
To date, eight laboratory science education programs have licensed access to our digital database of hematology slides. The database represents a resource for instructors who have already developed hematology courses and is a repository of learning objects. Future directions will include continuing education modules and the development of a digital curriculum supported by the database for a complete hematology course online.
References
1. Zhao Y, Lei J, Yan B, Lai C, Tan HS. What makes the difference? A practical analysis of research on the effectiveness of distance education. Teachers College Record. 2005;107(8):1836-84.
2. Schoenfeld-Tacher R, McConnell S, Graham M. Do no harm - A comparison of the effects of on-line vs. traditional delivery media on a science course. Journal of Science Education and Technology. 2001;10(3):257-65.
3. Sitzmann T, Kraiger K, Stewart D, Wisher R. The comparative effectiveness of web-based and classroom instruction: A meta-analysis. Pers Psychol. 2006 Fal;59(3):623-64.
4. Bernard RM, Abrami PC, Lou YP, Borokhovski E, Wade A, Wozney L, et al. How does distance education compare with classroom instruction? A meta-analysis of the empirical literature. Rev Educ Res. 2004 Fal;74(3):379-439.
5. Selected Occupational Projections Data. 2010 05/19/2010; Available from: http://www.bls.gov/ooh/
6. Regan, M. and R. Forsman, The impact of the laboratory on disease management. Dis Manag. 2006. 9(2): p. 122-30.
7. Brueggeman MJ, Swinehart C, Yue MJ, Conway-Klaassen JM, Wiesner SM. Transitioning to virtual instruction in clinical hematology teaching laboratories. Clin Lab Sci. In Press.