Background Information
As with all methodologies within the medical laboratory, Hemostasis testing has evolved considerably over the past 50 years. Testing methods in this discipline have changed from the original coagulation tilt-tube methods of the 1960s and 1970s to semi-automated methods (e.g. Fibrometers), and now to fully automated methodologies. However the fundamental principles used in the methodologies have remained relatively static during these same years. Campus laboratories needed to evolve to prepare students for current practice methods, but many semi-automated coagulation instruments that we traditionally used for campus instruction are no longer in production and the expense of current fully automated instrumentation is beyond the reach of many educational programs. Our first concern was therefore lack of funding to provide students with access to the required instrumentation for these tests. The second problem we faced was that our program had also recently opened a second performance site at a coordinate campus. Because we are accredited as a single program, we needed to insure that the education provided to students at the second location was equivalent to the instruction at our original location.
Understanding of reagents and implications of results for patient management are essential for student competency in Hemostasis. For our program’s student laboratories, on-campus instruction involves manual or semi-automated methods, so that students can “see” what is occurring during the testing method. It is also essential that students understand what is being done inside the instrumentation as they move from campus, to their clinical experiences, and eventually into the workplace. Knowledge of the methodologies allows them to detect potential errors, troubleshoot instrument malfunctions, validate instrument performance, and eventually evaluate and interpret patient results.
Because the majority of Hemostasis testing in hospital laboratories is currently performed on automated instrumentation, students no longer needed to develop any proficiency in performing the manual method. Nevertheless, visualization of this basic method has instructional value toward understanding the underlying analysis. Many of the hands-on skills used in this discipline were also taught in other portions of our curriculum. We therefore decided to investigate the possibility of developing a virtual experience in this subject area to teach the fundamentals of pathophysiology and diagnostic testing theories without a wet laboratory, while using a technique that allows the student to directly visualize the reactions detected using current instrumentation.
Several factors influenced our shift to virtual laboratory exercises for Hemostasis:
- lack of instrumentation, reagents, and supplies for student laboratories within our budget
- the need to provide equivalent instruction at two locations
- current Hemostasis practice does not require the psychomotor skills associated with manual or semi-automated coagulation testing
- the skills that are required are provided in other courses in our curriculum
Developing the Virtual Laboratory Exercises
In 2005, as the CLS Program was reorganized into the Center for Allied Health Programs, we faced the need to replicate our curriculum at the Rochester coordinate campus. Although some funding was provided for this expansion there was not enough to purchase duplicate instrumentation for the student laboratories as well as reagents and supplies. The lead faculty member had also attended a session on campus in which a laboratory course was demonstrated containing similar skills and activities required in our laboratory course. She then began to explore the potential of developing a virtual laboratory course for this topic area.
The target for our online course project was five Hemostasis laboratory exercises traditionally taught using manual methods and their corresponding face-to-face didactic lectures. Before proceeding on this project it was essential for us to determine whether these course units could truly be presented in a constructive manner through online delivery format. Before initiating the project CLS Program faculty met with an instructional designer versed in developing virtual exercises for students. A critical phase of the development was to generate a “storybook” rendition of the didactic content as well as for the steps involved in the laboratory exercises. Faculty acted as the content experts for this process and worked directly with instructional designers to fully outline the course and individual exercises within the course. This took a lot more effort and time than expected but was essential for our success. By working with “non-expert” instructional designers, CLS faculty were forced to reflect in great detail about the steps involved in teaching the material, what was expected from students as they entered this course and what terminal goals were involved. Only then could we develop a strategic process for developing the online modules to help student reach the competencies needed. After agreeing on the basic template the faculty worked with a team versed in online education module development including an instructional designer, videographer, and an Adobe® Flash programmer to develop a virtual laboratory session for each of the existing traditional laboratory exercises and corresponding lectures.
Screen-by-screen module content was developed by our program faculty using PowerPoint® or Microsoft Word®. These screens were then converted to Adobe® Flash by a contracted programmer. Because we had invested a significant amount of time in developing the detailed storybook for each exercise, instructional designers were able to help us align the course materials in an appropriate sequence directed toward the expected student outcomes. For our particular project, this meant rearranging some of the content along with some minor enhancements (more in-depth explanations) but no material was added or deleted from the original course. Based on the instructional goals they helped us develop appropriate assessment tools for the exercise outcomes. The first module took approximately 4 months to develop, however the additional modules took far less time because many of the activities were similar between the modules. The lecture and laboratory lessons were divided into the following virtual lecture/laboratory modules:
- Prothrombin Time (PT)
- Activated Partial Thromboplastin Time (APTT)
- Thrombin Time (TT)
- Factor V Assay
- APTT Inhibitor/Inactivator Assay
In each of the exercises, the students went through the entire traditional process including reconstituting and mixing reagents, confirming water bath temperatures, gathering all testing supplies, etc. Instead of simply watching a video of someone performing the testing, these modules required student interaction. The student had to select the reagents from materials on the screen using a computer mouse, mix the reagents, check water bath temperatures and set up each test tube. The student then performed the clotting test online by starting a stopwatch when reagent was added, watching a video of a clot forming and clicking the stopwatch again when the video showed clot formation. In our current application, students downloaded and filled-in a worksheet for each exercise. Results were submitted through the online course management system for scoring. The instructional designers were extremely helpful in identifying where a picture or video would be helpful, when a knowledge check was needed, or when to have the student demonstrate a skill.
Students were allowed to practice as many times as they wished before testing their specimens and submitting their results. Even after their results had been submitted students could return to the modules for review and preparation for exams. This feature of extended practice was not available to the traditional delivery format students due to need for live laboratory time and the cost of reagents.
Support and Funding
Our educational program is housed within the Center for Allied Health Programs which was developed by the University of Minnesota’s Board of Regents in July 2006. The principles that created this new model included non-traditional models of delivery (hybrid education), learner‐ centered, leveraging technology, statewide access and outcomes‐monitoring. The proposed features involved technology learning platform and support to faculty to create a new online and hybrid curriculum. For these reasons, our program had a strategic initiative toward the use of technology in the delivery and enhancement of the educational curriculum. Funding support from the Director of the Center for Allied Health Programs and from the Vice President of the Academic Health Center who oversee our unit was an essential component to its development and implementation.
Comparison of Traditional and Virtual Delivery Student Outcomes
Because we are in an accredited medical program, we needed to verify that the use of this new delivery process was at least equivalent in student outcomes to the previous delivery model. The efficacy of this new delivery format was investigated by evaluating the performance of 272 students from our academic program over six years. A total of 101 students received Hemostasis instruction via the traditional face-to-face lecture and laboratory format (years 2006-2008) while 171 students received instruction via online lectures and virtual laboratory format (years 2009–2011). Exam questions during this six year time period were evaluated for their appropriate use in the study. Over the six-year span of instruction, only 13 questions were unchanged and consistently used on the Hemostasis exam without any modifications (Table 1). Student results were compared based on their course delivery format, using the “percent correct” on the individual test question items and performance on the Board of Certification (BOC) sub-discipline as the expected student outcomes. A comparison of GPA by student cohort year and by delivery format found no significant differences indicating there was no need to control for student GPA in our analysis of student outcomes.
Table 1: Student Performance on Exam Questions (percent correct)
| Question | Question Subject | Traditional | Virtual |
| 1 | Prothrombin times purpose | 73.3 | 75.3 |
| 2 | Use of Thromboplastin | 84.2 | 96.5 |
| 3 | Phospholipid function | 87.1 | 99.4 |
| 4 | Calcium function | 75.3 | 92.9 |
| 5 | Non-activated partial Thromboplastin time | 91.1 | 89.4 |
| 6 | Thrombin time | 90.1 | 91.8 |
| 7 | Factor VIII deficiency | 89.4 | 95.3 |
| 8 | Inhibitor/Inactivator study Case Study 1 | 84.6 | 83.9 |
| 9 | An abnormal PTT correction | 90.0 | 87.5 |
| 10 | Inhibitor/Inactivator Case Study 2 | 80.6 | 75.6 |
| 11 | Heparin Concentration Calculation | 75.8 | 91.2 |
| 12 | Factor Assay Interpretation | 86.2 | 95.9 |
| 13 | Factor Assay Procedure | 78.0 | 87.1 |
The overall mean percent correct on the 13 questions was higher for the virtual delivery student group (M=89.4%) compared to the traditional delivery student group (M=83.7%). The mean percent correct for the traditional delivery student group seemed to remain static while the mean for the virtual delivery student group seemed to be increasing (Figure 1). A t test was performed to compare the number of test items correct on the Hemostasis exams and student performance on the related sub-discipline on the BOC exam. Student cohort scores on the BOC showed no significant differences between the course delivery formats while a significant difference was found for student performance on the on-campus test questions. Since student performance on the BOC was not significantly different we have shown that this method of delivery can achieve the required student learning outcomes supporting continued use of this method of instruction in our program.
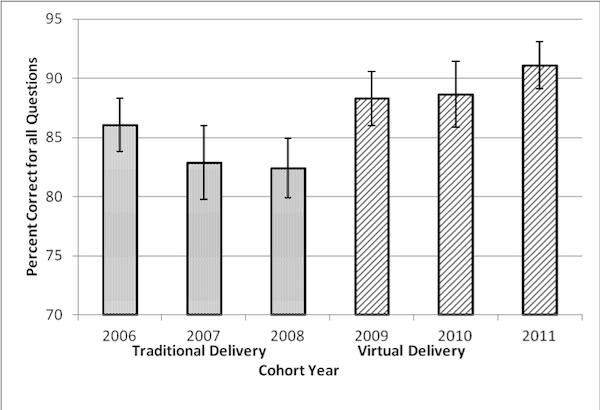
Figure 1: Students’ Average Exam Scores (Percent Correct) by Cohort Year
Analysis of Survey Results
Sixty five of the 171 students (38%) in the virtual delivery group completed the optional survey. Four students experienced some technical difficulties such as slow loading or screen freezes, but these students were connected to the Internet via phone modem. None of the students connected by cable modem or via digital subscriber line (DSL) reported having any loading or connection problems.
The vast majority of students (97%) felt that the virtual delivery was effective, provided confidence in understanding, and was easy to navigate. Students stated that they liked the ability to work with the modules at any time of day or night (48%) as well as the ability to repeat the modules multiple times (16%). They felt the ability to repeat the units along with the interactive nature helped build confidence in their understanding of the content and testing method (16%). They also felt that the online modules were straight-forward and concise and helped them focus on the content and purpose of the lesson.
Lessons Learned
During this process there were several lessons learned before, during and after the development of the online learning modules.
- The work with instructional designers helped set the stage for a student-focused delivery of course materials. It was critical for these individuals to help us strategically align the unit objectives with course materials and in turn the activities and assessments.
- In spite of having a fully developed course in place it took about 4 months to design the course for optimal student learning and then develop the web based modules. Things that are done in person, perhaps somewhat automatically by the instructor, have to be overtly integrated into an online course because the instructor is not there to add the explanation as students go along.
- An individual with expertise in Adobe Flash programming who could devote 100% of their time toward implementation, kept us on track toward meeting deadlines.
- From the student surveys, it became evident that with the conversion of curriculum materials to an online instruction and virtual laboratory exercise format, we not only needed to specify the minimum technical requirements for student computers but how they access the Internet as well. The size of most image and video files were too large for phone modem access, causing problems for some students. This may also limit accessibility to rural areas experiencing critical shortages of trained personnel and thus the possibility of expanding to more rural coordinate campuses in the future until adequate high speed Internet infrastructure is developed. During the last year of the study and for the future, the program required students to have access to either cable or DSL connections to the Internet as part of the admissions requirements.
- Complete course conversion to a digital simulation format is rarely contemplated years in advance. Lack of anticipation of the availability of funding and expertise to accomplish this project limited the vision of program faculty regarding course redesign possibilities. As a consequence, adequate care was not taken in the collection and preservation of student performance data and we were forced to rely on aggregate data rather than on individual matched datasets. A more comprehensive approach to data collection and storage has been implemented so that studies will not suffer the same limitations at our institution in the future.
Summary
Many universities and health science programs in particular have embraced the development of online education and virtual laboratory experiences to enhance student learning and expand access. In this study we developed a set of virtual lecture and laboratory exercises to replace traditional wet laboratories and face-to-face lectures. Although literature has shown that students in online instructional delivery formats reach equivalent outcomes to students in traditional delivery formats, it was essential that as an accredited allied health program, we evaluate the efficacy of this new delivery format on our student and program outcomes. The success of this project encourages us to explore other areas of laboratory science education which could be converted or enhanced through application of digital learning models.
References