Sections of this paper were previously presented at EDULEARN11 Conference, July 2011, Barcelona, Spain [11].
Introduction
Medical education in North America has been influenced by Carnegie Foundation sponsored studies twice in the last one hundred years. The first study was conducted in the early 19th century by Dr. Abraham Flexner, who visited all 155 US and Canadian medical schools operating at that time [ 1 ]. A ‘2+ 2’ medical school curriculum subsequently emerged, whereby two years of classroom instruction in scientific foundations were followed by two years of clinical experience. Recognizing that knowledge has grown, systems have changed and understanding of learning has advanced since 1910, a more recent study of 11 medical schools was conducted, culminating in the report Educating Physicians: A Call for Reform of Medical School and Residency [ 2 ].
This 2010 report heavily promotes integration, habits of inquiry, and formation of professional identity, while acknowledging the quality-maintaining role of accrediting and licensing bodies, such as the Liaison Committee on Medical Education (LCME). Coincidentally, Call for Reform was issued just as the University of Minnesota Medical School (UMNMS) prepared for a 2012 accreditation visit by the LCME. Motivated by the report’s vision of medical education of the future and “intrinsically…by the desire to improve student learning”, UMNMS set out to revise its curriculum to prepare its students to practice 2nd millennial medicine.
Challenges
Per (backward) course design [ 3 ],an examination for salient situational factors is the critical first step, and indeed, designers and developers of the revised UMN curriculum identified several challenges.
To meet accreditation standards. To be granted full accreditation status for an eight year cycle, medical schools must meet over 120 standards. But accreditation is more than a quality assurance process. Accreditation has implications for both school and student, as full status establishes medical school eligibility for federal grants and is a condition for medical student licensure upon graduation [ 4 ]. In other words, there would be consequences should the UMNMS not maintain its accredited status.
To preserve a lifetime of work. Standards ED 5A [ 5 ] and ED 33 [ 5 ] are central to this story. ED 5A specified opportunities for active learning and independent study whereas ED 33 specified content integration within and across periods of study. Meeting standard ED 5A posed a challenge, as per the conventional ‘2+2’ model, the Years 1 and 2 scientific foundation UMNMS courses have been isolated from clinical experiences and dominated by lectures. In spite of the known advantages of active learning, such as longer knowledge retention [ 3 ], faculty were reluctant to discard their lifetime of work and source of pride. Having invested years to iteratively develop reusable lecture slide decks and faculty authored primers, there were concerns about ‘starting from scratch’ to develop new instructional materials for independent, integrated and interactive learning i.e., if there was a call to abandon lectures, it would cause a shock wave. Finally, to integrate content between the basic and the clinical sciences and between single organ specialties, the challenge would be to break through organizational ‘walls’ separating divisions and departments, reinforced by decades of independent habit carried over from the clinical world.
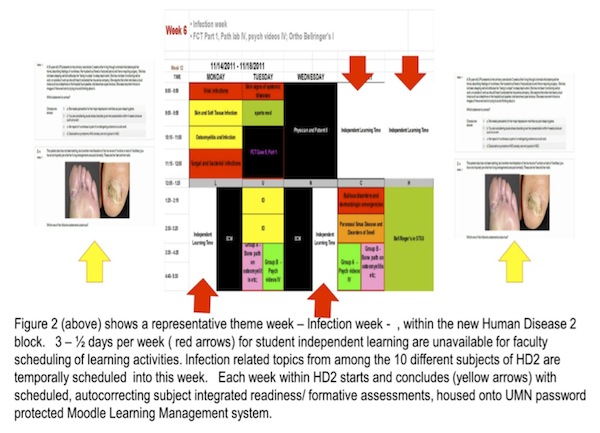
To make room in the schedule. To date, the Years 1 and 2 UMNMS calendars had classes / laboratory sessions scheduled daily, from 0800 h to 1730 h, with one hour for lunch and ten minute breaks between classes. To promote student independent study, and preparation in advance, the UMNMS curriculum scheduled 3 half days of Independent Student Learning Time (ILT) per week into Years 1 and 2, effective August 2010 (Figure 2 – red arrows). This meant reducing the number of hours available for classroom-based instruction from 40 to 20 hours per week.
To optimize limited facilities and faculty numbers. Interactive small group seminars can be an effective strategy to shift classroom focus to application of knowledge. But to offer these to a class of ~ 180 students, in place of lectures, more trained faculty facilitators and more small group rooms would be needed. Seminar rooms with wireless upgrades, however, are in demand by the other six health- oriented UMN Academic Health Center schools, also advocates of active learning in the pre-clinical years of training.
Basically, we had our work cut out for us, as to introduce new active learning activities for more effective learning into a reduced 20 hour weekly schedule using limited resources would require optimizing ILT and finding other non-small group seminar instructional methods.
How it was done
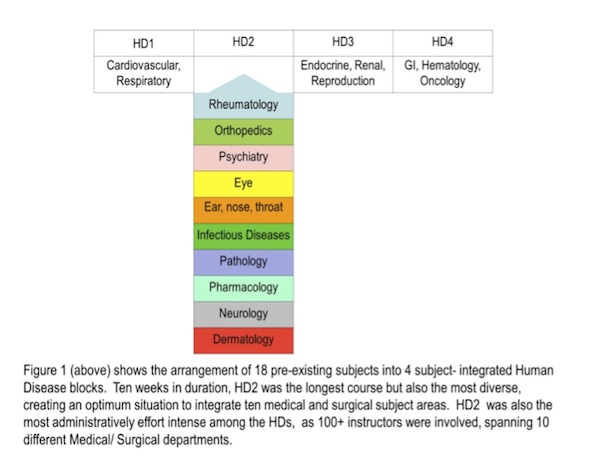
Starting at the curriculum level, and focusing on Year 2, Medical School curriculum leadership regrouped the original 18 Year 2 subjects into four Human Disease (HD) blocks to promote the integration of basic sciences with clinical subjects (Figure 1). This rearrangement included scheduling of ‘study weeks’ after each of 4 HD blocks instead of after every subject course, sparing individual subjects from having to sacrifice instructional time as a result of the restructure.
Next, we zoom in on Human Diseases 2 (HD2) block, the primary goal of which is to prepare the student for the heavily clinical 3rd year of their medical school training in the HD2 member subject areas. Drawing upon the lessons and experience as an Education Technology Faculty Fellow and leveraging the relationship between the author/ HD2 course director and the UMN Collaborative for Academic Technology Innovation [ CATI ] were key to the transformation of challenges into opportunities and to the design of a course that achieved its primary goal. CATI consultants have
- An expertise in educational technologies emerging both within and outside of the UMN,
- An expertise in the pillars of adult learning and instructional design and
- A long track record of faculty development offerings (e.g. OIT Education Technology Faculty Fellowship Program).
Next, these principles to guide the design of HD2 were established:
- Eliminate duplication of material that appears in more than one subject area within HD2,
- Goals and objectives to be learner-centered; instruction to respect the students’ baseline level of knowledge and skill,
- Identify faculty development opportunities and educational technologies matched to faculty/ staff skill levels and to instructional needs and where suitable, upgrade existing materials for long term use,
- Accept initial imperfection, but iteratively improve by welcoming and incorporating program evaluations.
The result is a collection of examples showing how education technology operationalized models and frameworks to meet the new curricular requirements of integration, interactivity and independent learning.
Example 1: MOODLE + ‘ladders’. MOODLE (or Modular Object Oriented Dynamic Learning Environment ) is free, open source, web based and intuitive to learn to use by students and faculty developers alike. UMN hosting provided password protection and technical support. This learning management system helped make the ‘temporal integration’ rung on Harden’s integration ladder [ 6 ] more interactive: the nine instructional weeks of HD2 became a series of ‘theme’ weeks, each week bracketed by MOODLE based electronically scheduled, autocorrecting, readiness/ formative questions (Figure 2) based on learning objectives for the respective week.
Finally we zoom in further to the level of the Rheumatology subject, within HD2. In the broadest sense, Rheumatology is the specialty that a) diagnoses and non-surgically manages joint damage (e.g. osteoarthritis) and b) investigates and manages diseases where the process of raging inflammation (e.g. lupus, vasculitis….) can damage any organ (brain, lungs, eyes, kidneys, skin…). The medication arsenal a rheumatologist uses varies from steroid injections into inflamed joints to immune system taming antimalarial drugs to organ salvaging chemotherapy, even if cancer is not the diagnosis. These potent medications also have potential side effects, likewise not limited to any one organ. In other words, integration is not a challenge to the rheumatologist, as their thinking is not limited by ‘silos’. Rather, small divisions, such as Rheumatology, do not have the luxury of recruiting the few clinical faculty away from patient care responsibilities in order to do what they also love, teach, especially when patient appointment backlogs exceed 3 months. For the faculty rheumatologist, the challenge of introducing new active learning activities for more effective learning into a reduced 20 hour weekly schedule using limited classroom resources has significant patient care implications. Fortunately and once again, educational technologies came to rheumatology’s aid to operationalize models and frameworks and ensure that new curricular requirements of integration, interactivity and independent learning are met, without having to cancel patient appointments.
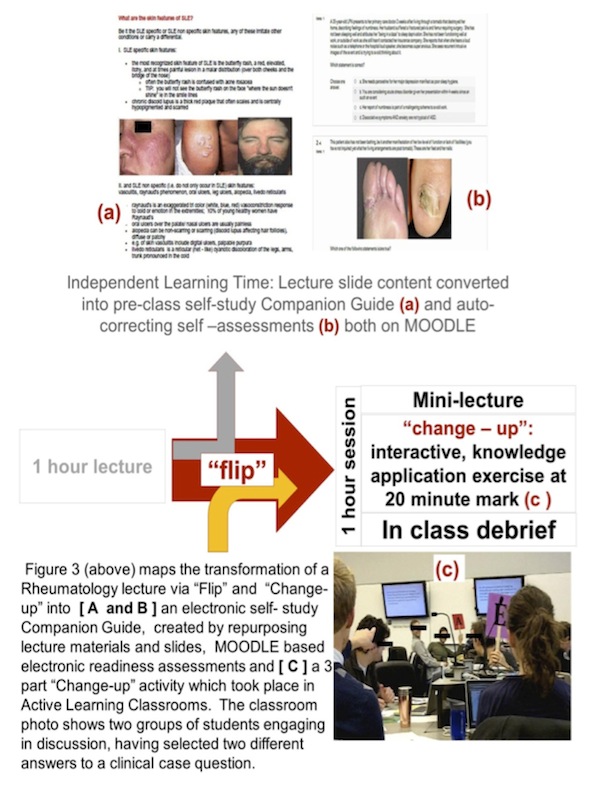
Example 2: MOODLE + ‘flipped classrooms’. Working within faculty time and scheduling constraints, but still guided by the learner centered design principles, Rheumatology boldly did the unthinkable, abandoning lectures and ‘flipping the classroom’ [ 7 ]. The 3 – ½ days per week of Independent Learning Time were leveraged to “free up… class time for experiential …activities, (and became an) alternative way of introducing students to the key information and ideas of the course, i.e., the content.” [ 3 ] Rheumatology elected to repurpose its original 7 – 1 hour lecture slide decks into a faculty authored student self- study Companion Guide, posted onto MOODLE. Assigning students to read sections of the Guide in advance of scheduled Rheumatology sessions and to answer MOODLE based readiness questions pre-class [Figure 3 a) and b) ], is an example of an education technology based strategy not infrequently used whereby “online quizzes with immediate feedback and the ability to rerun lecture segments may help clarify points of confusion” [ 7].
Example 3: MOODLE + ‘flipped classrooms’ + ‘change- up’. With Rheumatology lecture slide decks repurposed as MOODLE posted Companion Reading Guides, paired with MOODLE readiness questions, the 7 individual hours of class time were now available for active learning, clinical reasoning and knowledge application exercises. Rheumatology chose to follow the 3 part ‘change –up’ model [ 8 ] as each step served important educational purposes.